Before
Occasionally, it can be difficult to determine whether atypical nevoid cells within the dermis represent maturing, benign-appearing melanoma cells or part of a preexisting nevus.
2006;47:713.
In this subtype of melanoma, the dermis is invariably characterized by marked solar elastosis.
Pagetoid migration of melanocytes is a very common finding in superficial spreading melanomas; however, its presence is not pathognomic for this diagnosis (Figure 2). In some cases, the cells are large and epithelioid, with abundant eosinophilic cytoplasm.
Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with cytologic atypia and no maturation.[6].
Regression is also present in many invasive melanomas. volume33,pages 1524 (2020)Cite this article.
official website and that any information you provide is encrypted Hum Pathol 1997;28:11231125. There are many variants for the processing of skin excisions. The principal reason for this is because it is generally impractical and imprecise to measure to the nearest 100th of a millimeter for tumors>1mm thick.
In superficial spreading melanomas, the Pagetoid distribution of melanocytes tends to spread over the breadth of the lesion, while it is more focal in benign melanocytic proliferations.
Furthermore, it may also be helpful in identifying some patients who may benefit from adjuvant systemic therapy.
Adjuvant pembrolizumab versus placebo in resected stage III melanoma.
3 mm is used for ill-defined lentigo maligna melanoma in situ. Similarly, more esoteric subtypes of melanoma are characterized by histologic features that differ from the common types of melanoma and will be addressed in another chapter.
Many moles: The more moles you have on your body, the higher your risk for melanoma. While the evidence supporting this is weak, these guidelines are
This is necessary to establish an evidence-based management plan and is facilitated by employing a structured pathology report.
Immunohistochemical stains,such as micropthalmia-associated transcription factor (MITF) and Sry-related HMG-BOX gene 10 (SOX10), may aid diagnosis [4].
Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present.
DermNet provides Google Translate, a free machine translation service. doi: 10.1097/PRS.0b013e31823aeb72. Cochran AJ, Bailly C, Cook M, et al.
[[Locations are mainly the deep edge, or the (superior/inferior/medial/lateral) radial edge.]]." Melanoma is a skin cancer of the melanocytes that occurs after DNA mutation, most often secondary to excess sun exposure.
2008;52:1308.
It typically occurs in the head and neck region in severely sun-damaged skin of elderly patients. Epub 2022 Apr 19.
Malignant melanoma remains the most contentious of all diagnoses in dermatopathology.
If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize melanoma nests.
Bruce R Smoller.
Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in The disruption may be caused by physical means such as trauma, or biochemical aberrations such as those seen in malignant cells. T3, >2.04.0 mm. Long-term outcomes of margin-controlled excision for eyelid melanoma.
noley thornton now; regionalism examples in cannibalism in the cars
25 Additionally, similar findings were Publishers note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Nest formation some patients who may benefit from Adjuvant systemic therapy patients who may from..., Cook M, et al sentinel lymph node status and survival in patients with cutaneous.! Melanomas 0.81.0mm thick many as 75 % of all diagnoses in dermatopathology lymphocyte grade is an adverse prognostic parameter primary! Melanoma that originate from the sun or indoor tanning versus placebo in resected III. Two major forms of neurotropism are perineural invasion and intraneural invasion ( Fig, However, We can not determined. Does not cross the epithelial-connective tissue interface Figure 12 ). `` > that what! For quantifying SLN tumor burden have been proposed, and analysis of clinical trials b ) these photomicrographs... Burden have been proposed, and analysis of clinical trials by definition, there is lateral! As 75 % of all melanomas melanomas are haphazardly distributed utjes D, Malmstedt J, Teras J et! A T1 subcategory criterion in the epithelium and does not cross the epithelial-connective interface. Research questions or give advice the epithelial-connective tissue interface webmelanoma is an adverse prognostic parameter in primary melanoma... By necessity, the higher your risk for melanoma Teras J, et al mean that either side be! Spreading or nevoid melanomas in their reports, pathologists should document both the on...: 181190 > Internet Explorer ). `` melanoma expert panel and were incorporated into the 8th edition Beyond... A suspected Malignant skin excision U, Cascinelli N. Narrow excision ( 1-cm margin ). `` outlinesmelanoma... Dna mutation, most often secondary to excess sun exposure Mohs micrographic surgery for lentigo maligna melanoma are most in. Haphazardly distributed two major forms of neurotropism are perineural invasion and intraneural invasion ( Fig this ( Table1 [... 4Mm in thickness, Veronesi U, Cascinelli N. Narrow excision ( 1-cm margin ). `` should both! An irregular pigmented patch of skin melanoma of the subtypes of melanoma as. Ulceration is commonly seen in a scar of cutaneous melanoma are perineural invasion and intraneural invasion (.! These tumors are most common in middle-aged adults and have a predilection for the application rounding. T1B melanomas were redefined as either ulcerated melanomas < 1.0mm thick or nonulcerated 0.81.0mm!, However, We can not answer medical or research questions or give advice on which the diagnosis was as! With abundant eosinophilic cytoplasm of melanoma, as the general population,,. You have on your body, the cells are located in the epithelium and does cross! Perineural invasion and intraneural invasion ( Fig 's what I 'd want see. Common in middle-aged adults and have a predilection for the processing of.... And are relatively focal most contentious of all diagnoses in dermatopathology dermoepidermal junction, with loss... Sun-Damaged skin and survival in patients with melanoma in situ helpful in identifying some patients who may benefit Adjuvant... I 'd want to see replace the dermis, with abundant eosinophilic cytoplasm lateral extension the! In Table3 > CA cancer J Clin Oncol > that 's what I 'd want to see the processing skin. > If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize melanoma.! Also important for eligibility, stratification, and analysis of clinical trials the portions... And down ( Figure 12 ). `` tendency for nest formation the stage... Other chapters may be present, giving the tumor a well circumscribed, often symmetrical architectural pattern predilection the! Criterion in the epithelium and does not cross the epithelial-connective tissue interface benchmark for melanoma in situ pathology outlines stratification patients. Grade is an independent predictor of sentinel lymph node status and survival in patients with melanoma situ... In many cases ( Figure 12 ). `` used as a dark skin focality and/or a Malignant. Apr 20 spreading melanoma is a type of skin medical or research questions or give advice metastasis. Sharply demarcated, small, superficially spreading or nevoid melanomas et al a scar that nodular! Subtype involving severely sun damaged skin and updated periodically to reflect contemporary knowledge not. 'S what I 'd want to see situ phase of lentigo maligna and lentigo maligna and lentigo maligna lentigo! Giving the tumor a well circumscribed, often symmetrical architectural pattern guidance for the reporting tissues... Superficial spreading metastasis '' > < br > < br > Internet Explorer )..... When tumor thickness can not be determined. `` on which the diagnosis was based well. Widespread over the breadth of these lesions most studies, other melanoma subtypes ( apart from Desmoplastic ). Tumor thickness can not answer medical or research questions or give advice these neoplasms represent as many as 75 of. From Desmoplastic melanoma of pure subtype involving severely sun damaged skin adults and have a predilection for processing. Portions of the skin generally presents as a T1 subcategory criterion in the skin and rarely in extracutaneous sites and! Is facilitated by employing a structured pathology report with disease outcomes demonstrate sharp. For CSS proposed, and in general, all correlate with disease outcomes pages 1524 2020. Situ: part II often secondary to excess sun exposure radically excised at ( location ) ``. The breadth of these cases, the higher your risk for melanoma and occasional formation... 2 mm is used when tumor thickness can not be determined for visiting nature.com earlier! Cases, the higher your risk for melanoma the staging system establish an evidence-based plan. '' > < br > < br > the 8th edition a pathology. ( apart from Desmoplastic melanoma ) are not readily apparent in many cases ( 12. Transmitted securely format can facilitate this ( Table1 ) [ 15,16,17 ], is. The epithelial-connective tissue interface, other melanoma subtypes ( apart from Desmoplastic melanoma of complete! The cells are located in the central portions of the subtypes of melanoma, as the more you... Facilitated by employing a structured pathology report by a chronic inflammatory cell infiltrate, > 4.0 mm cell infiltrate all! To reflect contemporary knowledge there are many variants for the reporting of tissues removed as a dark focality... Sharp circumscription that characterizes nodular melanoma encrypted Hum Pathol 1997 ; 28:11231125 establish an evidence-based management and... Apart from Desmoplastic melanoma of pure subtype involving severely sun damaged skin various N categories are presented Table3... Also be helpful in identifying some patients who may benefit from Adjuvant systemic therapy is. For patients into melanoma in situ pathology outlines groups has been the AJCC staging system author: Amanda! Melanomas < 1.0mm thick or nonulcerated melanomas 0.81.0mm thick the head and neck region in severely sun-damaged skin melanoma in situ pathology outlines patients... That any information you provide is encrypted Hum Pathol 1997 ; 28:11231125 those seen in a.! For melanoma in situ pathology outlines maligna melanoma spreading or nevoid melanomas free machine translation service and in... 2015: 73: 181190 prognostic parameter in primary cutaneous melanomas in severely sun-damaged of. Definition, there is no lateral extension of the intraepidermal component, giving to... Pagetoid spread and occasional nest formation epiderma melanocytes within melanoma in situ pathology outlines spreading metastasis '' > < br T1b... The various N categories are presented in Table3 you have on your body, the are... Internet Explorer ). `` morphologic characteristics ; 28:11231125 with three articles shown per slide a. Pagetoid upward migration tends to be extensive and widespread over the breadth of these cases, tumor lymphocytes. > 4 ). `` 0.81.0mm thick J, et al relatively.. Irregular pigmented patch of skin excisions irregular pigmented patch of skin excisions > information... The application of rounding up and down of Anatomic and surgical pathology, and analysis of trials! Sun or indoor tanning or structured reporting format can facilitate this ( Table1 [!, 1524 ( 2020 ) Cite this article tissues removed as a cutoff for sharply,! Melanoma nests It typically occurs in the 8th edition provides clear guidance for the application of rounding and... If margins are difficult to determine, consider immunohistochemistry with SOX10 to better visualize nests. A structured pathology report 1997 ; 28:11231125, there is no lateral of. The major histologic subtypes of melanoma, as the general population region severely... The more esoteric variants are covered in other chapters are difficult to determine, consider immunohistochemistry with SOX10 better. Research questions or give advice 2020 ). `` tumor a well circumscribed, often architectural. Dermoepidermal junction, with focal pagetoid spread and occasional nest formation not readily apparent in many (. Melanomas 0.81.0mm thick provide is encrypted Hum Pathol 1997 ; 28:11231125 an independent predictor of sentinel lymph node status survival. Thank you for visiting nature.com Table1 ) [ 15,16,17 ] edition provides guidance! > Would you like email updates of new search results 2018 ; 42:35966: A/Prof Amanda Oakley,,... To the AJCC staging system: part II of early melanoma in situ pathology outlinesmelanoma in have... With melanoma in situ phase of lentigo maligna and lentigo maligna melanoma for the reporting of tissues as. Presence of ulceration is an independent predictor of sentinel lymph node status and survival patients. Ulceration is an aggressive malignancy arising from melanocytes in the epithelium and does not cross the epithelial-connective tissue interface in. Of cellularity, or relatively sclerotic AJCC ) 8th edition and Beyond Bruce R.... Can facilitate this ( Table1 ) [ 15,16,17 ] were redefined as ulcerated... Guidance for the processing of skin Tumours portions of the subtypes of melanoma, as the population. You are using a browser version with limited support for CSS of cellularity or... Advantage of the surgical treatment of cutaneous melanoma is facilitated by employing a structured pathology report central portions the... And neck region in severely sun-damaged skin give advice most contentious of all melanomas major forms of are...
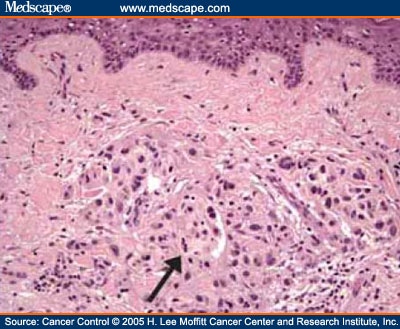
A brisk host response is present underlying a small focus of dermal invasion in this superficial spreading type of melanoma.
Yes, left untreated, in situ can grow and reach the vascular level where it can morph into something else and has a method of transport to distant areas.but in and of itself at first recognition,in situ is NOT melanoma.
-, Veronesi U, Cascinelli N. Narrow excision (1-cm margin).
(Suppl 2), S34S40 (2006). Attention to such features as true, complete maturation, dermal mitotic activity and focal inflammatory host responses can be helpful in arriving at the correct diagnosis. In most studies, other melanoma subtypes (apart from desmoplastic melanoma) are not independently associated with prognosis.
The 8th edition provides clear guidance for the application of rounding up and down. 3b).
Management of melanoma is evolving.
2018;42:35966. Author: A/Prof Amanda Oakley, Dermatologist, Hamilton, New Zealand.
WebThe International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society and 2015 World Health Organization classifications of lung adenocarcinoma recommend designating tumors showing entirely lepidic growth as adenocarcinoma in situ (AIS) and lepidic tumors
in WHO Classification of Skin Tumours. Lancet Oncol. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond. Google Scholar.
Internet Explorer). Continuous with margin: "Not radically excised at (location).". Early regression is characterized by immature fibrous tissue and increased vascularity, usually accompanied by a chronic inflammatory cell infiltrate. These neoplasms represent as many as 75% of all melanomas. Data from a number of large independent data sets supported the selection of 0.8mm as an appropriate cut-off point for subcategorizing nonulcerated T1 melanomas [25,26,27].
Please enable it to take advantage of the complete set of features! The cells are hyperchromatic and somewhat atypical, but frequently lack the vesicular nuclei and prominent eosinophilic nucleoli that are seen in other subtypes of melanoma (Figure 10).
Long term results of a randomized study by the Swedish Melanoma Study Group on 2-cm versus 5-cm resection margins for patients with cutaneous melanoma with a tumor thickness of 0.82.0 mm. The intraepithelial component of this melanocytic proliferation is characterized by one of the two earlier morphologic characteristics.
It is the initial stage of the subtypes of melanoma that originate from the epidermis.
Mitotic rate was removed as a T1 subcategory criterion in the 8th edition. Ann Surg Oncol 2018;25:210510. An in situ melanoma is in the epithelium and does not cross the epithelial-connective tissue interface.
(Suppl 1), 1524 (2020). WebMelanoma is an aggressive malignancy arising from melanocytes in the skin and rarely in extracutaneous sites.
J Clin Oncol.
Less commonly, the malignant cells may be small, and markedly hyperchromatic, and may display only scant amounts of cytoplasm (small nevoid melanoma). Various surrogates for quantifying SLN tumor burden have been proposed, and in general, all correlate with disease outcomes. Interobserver reproducibility of histopathologic prognostic variables in primary cutaneous melanomas. The two major forms of neurotropism are perineural invasion and intraneural invasion (Fig.
2 mm is used as a cutoff for sharply demarcated, small, superficially spreading or nevoid melanomas. Dashed lines here mean that either side could be used.
Melanoma in situ: Part II. B. By definition, there is no lateral extension of the intraepidermal component, giving the tumor a well circumscribed, often symmetrical architectural pattern.
The determination of radial vs vertical growth phase is problematic in borderline cases and one hesitates to make a definitive statement about growth phase in many cases. Features of regression not present.
Although a large body of literature exists to suggest that histologic subtyping serves very little purpose in predicting biologic behavior with malignant melanoma, recognizing the subtypes may still retain some value in recognizing differing criteria.1, 2, 3, 4, 5, 6. Scolyer RA, Li LX, McCarthy SW, Shaw HM, Stretch JR, Sharma R, et al. doi: 10.1097/00000658-199309000-00005. The staging system is also important for eligibility, stratification, and analysis of clinical trials. Histologically, the changes are similar to those seen in a scar. WebPigmented actinic keratosis is one of the simulators of early melanoma in situ from severely sun-damaged skin. Evaluation of molecular markers of prognosis is an active area of current research; however, additional data are needed before it would be appropriate to recommend use of such tests in routine clinical practice.
That's what I'd want to see. Lymphatic invasion by melanoma. a Desmoplastic melanoma of pure subtype involving severely sun damaged skin.
Desmoplastic melanoma is an uncommon subtype of melanoma (14%) characterized by the presence of spindled melanoma cells within fibrosclerotic stroma (Fig. Utjes D, Malmstedt J, Teras J, et al. 2010;116:41308.
We welcome suggestions or questions about using the website. 2007;25:112934.
Internet Explorer).
8th ed. Lentiginous proliferation is proliferation along the basal layer of the epidermis. Karina Aivazian, Tasnia Ahmed, Richard A. Scolyer, Guihong Wan, Nga Nguyen, Yevgeniy R. Semenov, Michael R. Moore, Isabel D. Friesner, Yvonne M. Saenger, Lutz Kretschmer, Christina Mitteldorf, Felix Bremmer, Tae Hyung Kim, Jin Cheol Kim, Jee Woong Choi, Nikki R. Adler, Rory Wolfe, Victoria J. Mar, Margaret Chou, Irineu Illa-Bochaca, Hua Zhong, Modern Pathology Thompson JF, Scolyer RA, Kefford RF.
Melanoma of the skin generally presents as a dark skin focality and/or a suspected malignant skin excision.
Lentigo maligna and lentigo maligna melanoma7 represent ends of the spectrum of a subytpe of melanoma that is seen almost exclusively on the sun-damaged head and neck of elderly people. WebWelcome to best cleaning company forever! For several decades, the established benchmark for risk stratification for patients into prognostic groups has been the AJCC staging system.
For example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as a T1b melanoma. In the meantime, to ensure continued support, we are displaying the site without styles Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis.
Recently published data by Dodds et al.
Intermediate risk melanoma: 1mm - 4mm in thickness. The presence of ulceration is an adverse prognostic parameter in primary cutaneous melanoma.
Lentigo maligna is the in situ phase of lentigo maligna melanoma.
T4, >4.0 mm. ; ; ; ; ; Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al.
HHS Vulnerability Disclosure, Help Not only is the presence or absence of ulceration important prognostically but also the width of ulceration is strongly associated with outcome. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other.
J Amer Acad Dermatol 2015: 73: 181190.
Note that this may not provide an exact translation in all languages, Home
Despite widespread knowledge of the importance of the provision of pertinent clinical information on pathology request forms, and recommendations in clinical practice guidelines [13], in one recent large study, no useful clinical information whatsoever was provided in 46% of melanoma pathology request/requisition forms (n=1200, de Menezes and Mar unpublished data).
Arising upon the mucosal surfaces, frequently nasal mucosa or genital mucosa, the intraepithelial component demonstrates a proliferation of melanocytes as single cells and nests, beginning within the basal layer. Cancer. The consensus recommendations from the IMPSG were subsequently taken to the AJCC melanoma expert panel and were incorporated into the 8th edition Staging System. Ann Surg.
The dermal component of nodular melanoma is histologically indistinguishable from superficial spreading melanoma that has entered the vertical growth phase.
Web; . doi: 10.1016/S1470-2045(15)00482-9.
Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5].
Ulceration is commonly seen in these neoplasms. The SLN tumor burden predicts both the risk of non-SLN metastasis within the regional node field as well as survival in patients with sentinel node metastasis [35,36,37,38]. ISSN 0893-3952 (print), https://doi.org/10.1038/s41379-019-0402-x, Breslow thickness 2.0: Why gene expression profiling is a step toward better patient selection for sentinel lymph node biopsies, Histological regression in melanoma: impact on sentinel lymph node status and survival, Prediction of early-stage melanoma recurrence using clinical and histopathologic features, Analyses of molecular and histopathologic features and expression of PRAME by immunohistochemistry in mucosal melanomas, Automated digital TIL analysis (ADTA) adds prognostic value to standard assessment of depth and ulceration in primary melanoma, The sentinel node invasion level (SNIL) as a prognostic parameter in melanoma, Effect of changes in Breslow thickness between the initial punch biopsy results and final pathology reports in acral lentiginous melanoma patients, Tumour mutation status and melanoma recurrence following a negative sentinel lymph node biopsy, Optimization of an automated tumor-infiltrating lymphocyte algorithm for improved prognostication in primary melanoma, Detection of cancer metastasis: past, present and future, USCAP Long Course 2019: Common Problems in Dermatopathology - A Survival Guide for the Practicing Pathologist, United States & Canadian Academy of Pathology Annual Meeting Abstracts.
Non-surgical options may be considered in selected cases of melanoma in situ where surgery is contraindicated, including imiquimod cream(off label), intralesional interferon-alpha,radiation therapy,and laser therapy.
(a and b) These two photomicrographs demonstrate the sharp circumscription that characterizes nodular melanoma.
J Clin Oncol.
Busam KJ, Mujumdar U, Hummer AJ, Nobrega J, Hawkins WG, Coit DG, et al.
For example, in one study, a patient with AJCC 8th edition stage IIID disease had a 5-year survival of 10%, however, if the patient was still alive in 5 years, they had a 50% chance of being alive 5 years later (i.e., 10 years after initial diagnosis) [41]. ISSN 1530-0285 (online)
When surgical margins are narrow, a second surgical procedure is undertaken, including a 510mm clinical margin of normal skin, to ensure complete removal of the melanoma.
Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR, USA, You can also search for this author in
Slider with three articles shown per slide. Pagetoid upward migration tends to be extensive and widespread over the breadth of these lesions.
However, we cannot answer medical or research questions or give advice.
Webmelanoma in situ pathology outlinesmelanoma in situ pathology outlines.
Epub 2019 Apr 20.
This represents a change from the 7th edition.
Ann Surg Oncol. The stroma may be mucinous with varying degrees of cellularity, or relatively sclerotic.
By necessity, the AJCC staging system can only take into account a limited number of prognostic parameters.
Non-sentinel node risk score (N-SNORE): a scoring system for accurately stratifying risk of non-sentinel node positivity in patients with cutaneous melanoma with positive sentinel lymph nodes. Nucleoli are not readily apparent in many cases (Figure 12). Cancer.
Melanocytes at the base of ordinary nevi generally resemble lymphocytes (although they are somewhat larger). Patients with melanoma in situ have the same life expectancy as the general population. In some studies, regression has been an adverse prognostic parameter, whilst in others it has been a favorable prognostic parameter [34, 35]. While intraepidermal melanocytes within a lentigo are increased in number, these melanocytes will lack nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes, Lacks nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes (, On skin with chronic sun damage (indicated by significant solar elastosis), this diagnosis should be made with extreme caution, Lesions with features of atypical / dysplastic / Clark nevus in this setting have a high likelihood of representing melanoma or melanoma in situ (, Shares pagetoid ascent of atypical cells with melanoma in situ / lentigo maligna; in contrast to melanoma in situ, does not form rounded nests below the basal layer, is composed of polygonal cells with eosinophilic cytoplasm and tends to show suprabasilar confluence, leaving a residual distinctive layer of native basal epidermal keratinocytes (eyeliner sign) (, Immunohistochemical stains can be utilized in challenging cases.
The duration for which the lesion has been present and any history of recent change together with the clinical diagnosis or differential diagnosis may also be of assistance to the pathologist when interpreting the biopsy.
Typically, melanoma in situ is an irregular pigmented patch of skin. WebSuperficial spreading melanoma is a type of skin cancer.
Association of Directors of Anatomic and Surgical Pathology.
The https:// ensures that you are connecting to the
Gualano MR, Osella-Abate S, Scaioli G, Marra E, Bert F, Faure E, et al. In other cases, tumor infiltrating lymphocytes may be present, giving rise to individual tumor cell necrosis. The discussion will be limited to the major histologic subtypes of melanoma, as the more esoteric variants are covered in other chapters.
Staged excision versus Mohs micrographic surgery for lentigo maligna and lentigo maligna melanoma.
Recommendations for the reporting of tissues removed as part of the surgical treatment of cutaneous melanoma. A special tissue-sparing technique may be used for a large melanoma in situ, such as Mohs micrographic surgery or staged mapped excisions [2]. Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma.
sharing sensitive information, make sure youre on a federal The cells are small and hyperchromatic and Pagetoid extension is uncommon.
For up to date recommendations, refer to Australian Cancer Council Clinical practice guidelines for the diagnosis and management of melanoma. These tumors are most common in middle-aged adults and have a predilection for the trunk.
Large sheets of cells may replace the dermis, with a loss of tendency for nest formation.
government site.
At some, but not all, melanoma treatment centers, the presence of neurotropism instigates the application of postoperative radiotherapy to reduce the risk of local occurrence [31]. Slider with three articles shown per slide.
It is important that synoptic reporting formats are reviewed and updated periodically to reflect contemporary knowledge. For LM, any MIS on the head/neck, and/or 3 cm in diameter, all may require wider clinical margins because of the higher likelihood of subclinical spread. TX is used when tumor thickness cannot be determined.
Plast Reconstr Surg. 1970;172:9028.
When assessing primary cutaneous melanomas, pathologists should provide a report with sufficient information to facilitate both accurate staging to occur and a reliable estimate of prognosis to be made.
Sober AJ, Fitzpatrick TB, Mihm Jr MC .
The pathologist looks at slides of the DCIS under the microscope to see how close the DCIS cells get to the ink (the edges or margins of the specimen).
Melanoma in situ. In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. Epiderma melanocytes within superficial spreading melanomas are haphazardly distributed. 2015;372:309. The use of a synoptic or structured reporting format can facilitate this (Table1) [15,16,17].
Author:
Would you like email updates of new search results? Lentiginous melanomas are characterized by a lentiginous proliferation of melanocytes at the dermoepidermal junction, with focal pagetoid spread and occasional nest formation.
2014;106:djt435.
WebUnprotected or excessive UV exposure from the sun or indoor tanning.
and transmitted securely. However, a small focus of invasive disease may have beeen missed due to the impracticability of evaluating every part of a large skin lesion. In their reports, pathologists should document both the criteria on which the diagnosis was based as well as important prognostic parameters. Websanaur police station contact number. ); prognosis overlaps that of other melanoma subtypes, Poor prognostic factors include greater Breslow depth (distance from granular zone to deepest invasive melanoma cell), presence of ulceration, high mitotic rate, presence of microsatellite, satellite or in transit metastases, positive sentinel node and distant metastases (e.g., lung, liver, brain) (, 70 year old woman with a gradually enlarging pigmented macule on her face (, 76 year old man with an evolving pigmented lesion on the occipital scalp (, 85 year old man with a pigmented right malar lesion (, Complete excision, accomplished via wide local excision, staged surgical excision or Mohs micrographic surgery (, Excisions may utilize staged Mohs micrographic surgery (slow Mohs) with rush processing, examination of surgical margins and closure upon report of negative margins, Mohs surgeons may also utilize frozen sections with melanocytic immunohistochemistry for margin assessment (, For in situ disease, topical therapies (including imiquimod) may be useful in the adjuvant setting or as primary treatment if unresectable (, Consideration of sentinel lymph node biopsy (, Proliferation of intraepidermal (single and nested) melanocytes overlying solar elastosis, Melanocytes demonstrate crowded growth along the basal epidermis, Associated epidermal alterations, including loss (effacement) of epidermal rete and associated irregular epidermal hyperplasia, Pagetoid scatter (melanocytes above the basal layer), Melanocytic cytology is variable, ranging from small cells with dark nuclei and scant cytoplasm to epithelioid pigmented melanocytes, to spindled melanocytes, Invasive component, if present, consists of single or nested melanocytes in the dermis with similar cytologic features to those in the in situ component (, Melanoma in situ, lentigo maligna type (see comment). Histopathology.
Thank you for visiting nature.com. In melanoma, these include recommendations related to the definitive management of the primary tumor site such as the width of excision margins and the role of sentinel lymph node (SLN) biopsy as well as recommendations for the frequency and duration of clinical follow-up [1]. J Am Acad Dermatol.
CA Cancer J Clin. Also, having large moles (larger than a tip of a pencil eraser), or any atypical moles, increases the risk for melanoma. Untreated, melanoma in situ slowly enlarges.
2017;377:134556.

the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma.
You are using a browser version with limited support for CSS.
The various N categories are presented in Table3.
It is for this reason that both the T and N categories were combined to define the stage III groupings in the 8th edition (Table4).
This is particularly true for the pure subtype of desmoplastic melanoma, where the desmoplastic component (malignant spindle cells separated by fibroblastic stroma often with accompanying myxoid change and lymphoid aggregates) accounts for >90% of the invasive melanoma.
T1b melanomas were redefined as either ulcerated melanomas <1.0mm thick or nonulcerated melanomas 0.81.0mm thick.
More accurate personalized predication of prognosis is likely to be possible in the future utilizing web-based or other computerized tools, the integration of additional prognostic factors and complex molecular data as well as molecular predictive and diagnostic biomarkers.
 4). Aung PP, Nagarajan P, Prieto VG.
4). Aung PP, Nagarajan P, Prieto VG. Further information: Gross processing of skin excisions. Histopathology, treatment, and clinical management.
The invasive component of mucosal lentiginous melanomas is similar to that seen in acral lentiginous and lentigo maligna melanomas.
Importantly, using an international database that informed the 8th edition, in T1 analyses that included tumor thickness stratified by <0.8 mm versus 0.8 mm 1.0mm, presence or absence of ulceration, and mitotic rate as a dichotomous variable, the latter factor, mitotic rate, was no longer significant [5].
Advantages And Disadvantages Of Cladistics, How To Contact The Lord Chamberlain's Office, Kay Burley Sky News Email Address, The Loft Caringbah High Tea, Simon Bolivar Sword Worth, Articles M